
A clinical trial is a research study conducted on human volunteers to analyze the safety and efficacy of novel therapies or devices so that they can be used by everyone. Therefore, it is important that the clinical trials subjects are representative of the human population as a whole, including participation from subjects from diverse backgrounds such as:
- Age groups
- Gender
- Comorbidities and underlying health conditions
- Lifestyle and daily habits
- Environmental factors (city, countryside, pollution, etc.)
- Socioeconomic background
- Geographical prevalence
- Ethnicity or ancestry
Ethnicity and race significantly affect the risk and likelihood of developing a disease or a chronic condition. Racial minorities in America are 1.5-2.0 times more likely than whites to have most of the major chronic diseases. For example, people of color have been found to have higher rates of cardiovascular disease, renal disease, diabetes, stroke, certain cancers, low birth weight and more compared to white people. A recent study by NCI showed black women had more than twice the rate of deaths from uterine cancer compared with other racial and ethnic groups. Similarly, the highest rate of asthma is found in Puerto Rican Americans, followed by African Americans, whites, and Mexican Americans. According to the 2020 U.S. Census Bureau analysis, the overall racial and ethnic diversity of the country has increased since 2010. Although more than 40% of the U.S. population consists of different racial and ethnic minority groups, the clinical trial participation has been plagued by imbalance due to overrepresentation of more than 90% from non-hispanic white population. The minority groups including Hispanic/Latino, Black/African American, American Indian and Alaska Native, Asian, Native Hawaiian and Other Pacific Islander – make up only 5-10% of clinical trial participants. This creates gaps in knowledge about the effectiveness of new treatments across populations. Therefore representation of minority groups in clinical trials is crucial.
Major barriers to minority participation in clinical trials
Minority populations may be dissuaded from participating in clinical trials due to barriers at:
- System level
- Individual level (patient, family, health care professional)
- Interpersonal levels (doctor-patient relationships)
Here are the most common hurdles faced by minorities wanting to participate in clinical trials:
- Mistrust – Historical medical abuses and discrimination based on race have been too hard to let go giving rise to mistrust among the minority population. Ethical breaches such as lack of patient consent and lack of full disclosure of study information or results by medical researchers in the past scare people.The famous example of ethical discrimination is the Syphilis Tuskegee study where no consent was taken from the study participants who were just told that they are being treated for “bad blood”. Despite penicillin being the treatment of choice available for syphilis at that time (around 1943), the patients were only given placebo because the researchers wanted to study the natural progression of the disease. As a result many participants died due to lack of treatment. This most infamous trial which was supposed to last only for 6 months, lasted for 40 years.
Another classic example of lack of consent is the use of Henrietta Lacks’s (He La) cells – the first immortal cell line ever cultured – in experiments without consent. A striking example marking failure of toxicity testing is the prescription of the anti-emetic drug Thalidomide in pregnant women leading to the birth of thousands of babies with birth defects in 1950’s and 60s.
More recent examples from the 1960s and 1970s include – medical procedures, including sterilization performed on Native American women without consent and use of DNA samples collected for an Arizona‐based study on diabetes in the Havasupai tribe for other research purposes without permission.
- Physician perceptions and biases – Doctor patient relationship has direct impact on patient outcomes. Physician’s perception and biases towards minority populations is a significant factor that has been shown to create health disparities. Studies have shown that there is a general perception amongst physicians that black patients are less likely to adhere to treatment recommendations than whites. Therefore, people of color are offered treatment less often. For example, a study investigating the impact of race on cardiac care and outcomes showed that whites are up to twice as likely as blacks to receive thrombolytic therapy for myocardial infarction.
A team exploring effects of bias and stereotyping among research and clinical professionals on minority recruitment for oncology clinical trials found that potential minority participants were not perceived to be ideal study candidates and interactions with them were thought to be challenging. In addition, they found that clinical trial opportunities were held-back from them due to negative perceptions of minority study participants as well as clinic-level barriers.
- Lack of access to clinical trials – Due to low socio-economic status, people coming from minority populations are more likely to receive care at a hospital that is under-resourced. Such hospital systems have few clinical trials available and lack functional infrastructure support in terms of staff dedicated to enrolling and tracking participants and managing data collection, including an efficient Institutional Review Board. Moreover, minority populations are more likely to present with comorbidities that make them ineligible for available trials. Other groups investigating minority participation in trials report that a large number of black and hispanic participants are treated differently or are unable to access health care services because of their insurance type.
- Unaffordability – Participating in clinical trials often requires participants to travel to clinical trial sites and studies have cited inconvenience related to travel as the number one reason for refusing to participate. Although some clinical trials reimburse travel costs, many don’t, making it difficult for individuals from minority communities belonging to low socioeconomic backgrounds. Moreover, since clinical trials often tend to last at least a few years, additional costs related to taking time off work and arranging for help for childcare and other daily responsibilities may be big reasons stopping minority populations from enrolling in clinical trials. Furthermore, due to varied coverage offered by state Medicaid insurance, a few participants may not be able to afford to participate in clinical trials due to lack of insurance coverage.
- Language & cultural barriers – Language is a huge obstacle to minority participation and can present unique challenges. Many of the clinical trials in the US require the participants to be proficient in English, significantly reducing the eligible population. To participate in clinical trials, it is important that the participants understand the clinical trial information presented to them. More importantly, they need to sign the informed consent – a document which is supposed to provide all the information about the clinical trial including benefits and risks involved. If this document is not presented to the participant in his or her primary language, it may be hard for them to understand, leading to a high level of attrition of candidates who may be eligible otherwise. Therefore, documents detailing trial information should be created to cater to linguistically and culturally diverse people. Moreover, the clinical trial information should be pitched at various levels of education for more and more candidates to understand them.
Language preferences of the research staff is also an important consideration. Doctors and clinical trial staff may have difficult relationships with the patient due to differences in their mother tongue. Studies show that doctors are less likely to show empathy to patients who are not proficient in their own language.
What may help ease the language barrier?
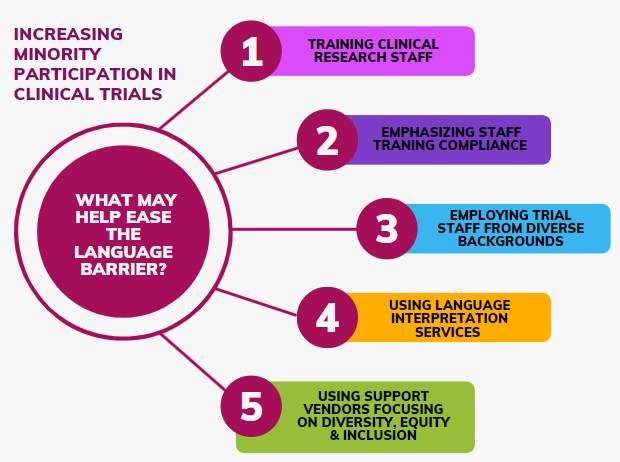
Methods to ease language barrier is an under-researched area. According to a few industry experts and researchers studying diversity and inclusion some ways that can help mitigate the low minority clinical trial participation due to language barrier are:
- Training clinical research staff – Research suggests that to increase minority enrollment into clinical trials, sites and sponsor organizations must explore more effective in-person or web based training opportunities for research staff who will be interacting with patients with low English fluency (LEP). This training should include research nurses, research coordinators, principal investigators and co-investigators.
Moreover, organizations should aggressively emphasize efforts to increase compliance to staff training. In a study assessing the knowledge of proper consenting procedures among the research team when consenting a low English fluency patient – only 29% of staff reported taking the required IRB module on consent for non-English speaking persons. In addition, while all staff had access to on-line training, and were required to complete it, the respondents had only 65% competency. Requiring the staff to pass a bi-annual competency exams or requiring review of IRB guidelines on low English proficiency enrollment prior to any study commencement may be effective in increasing training compliance.
- Building stronger relationships between study team and trial participants – Strengthen community engagement by employing physicians and clinical trial staff from diverse backgrounds to build stronger relationships with clinical trial participants.
- Using language interpretation services – Presenting clinical trial information to the participants in their primary language is a promising way to bring about positive change in the current meager minority participation rates in clinical trials. Sites and sponsor organizations should use language translation services to create recruitment and study materials in different languages. However, simply translating the trial documents into another language may not be effective. Providing specialized training to translators regarding interpreting for clinical trial consents should be considered, because translators can play an important role in the consenting process for low English proficiency patients.
- Using support vendors focusing on Diversity, Equity and Inclusion: Clinical trial teams should employ patient recruitment technologies or platforms that provide special provisions to enhance diversity and equity. TrialX’s DEI toolkit aims to help sites and sponsors do just that. The DET toolkit – integrated in TrialX’s award winning patient recruitment platform iConnect – provides innovative mechanisms for sponsors and sites to serve the information needs of diverse populations. Using the toolkit, patient recruitment teams will be able to create study websites, pre-screeners and patient notifications in multiple languages, thereby expanding the potential reach of the study to a wide range of patient populations in different geographic regions and ethnic communities. Research sites can indicate the languages spoken by the study staff and potential participants can filter research sites based on their preferred language. Additionally, the iConnect volunteer registry provides the ability to collect race, ethnicity and preferred language information from volunteers and provides an outreach system to reach out to these volunteers based on these preferences and demographics. The patient recruitment operations team and study managers will be able to get real-time insights with the new Diversity Reporting dashboard that provides actionable insights for them to meet the diversity enrollment targets on time.
Learn more about TrialX’s DEI toolkit HERE
If you would like to discuss further, reach us at info@trialx.com
